
Blood Types
In 1901, Austrian physician Karl Landsteiner discovered that there were different ‘types’ of blood. These blood types, A, B, and eventually O, made the practice of donation and transfusion significantly safer. The term most often referred to when discussing blood types is ‘compatibility’. But what about division? The discovery of blood types provided us with the ability to distinguish the blood of individual human beings and amplified existing beliefs in different kinds of blood. Our blood types can connect us with different people, yet at the same time, they can disconnect us from our friends, family, and other people.
The study of blood types’ geographical distribution reinforced beliefs amidst the hype of eugenics in the early twentieth century. In 1917-18, Polish-Jewish serologist Ludwik Hirszfeld and his wife, physician Hanna Hirszfeld, discovered that different ethnic groups had higher rates of certain blood types. More people living in the West had Type A blood, and more people living in the East had Type B blood. When eugenicists found out about the results of the Hirszfeld’s research, they used it to draw associations between blood types and ethnic heritage. They connected type A blood with Aryan traits and notions of ‘purity’, and type B blood with Jewish heritage.
Beliefs in blood type personality traits born out of popular eugenicist ideas of this time still enjoy popularity today.
In Japan, mascots which represent blood donation continue to feature references to different ‘blood personality types’.
Did you know?
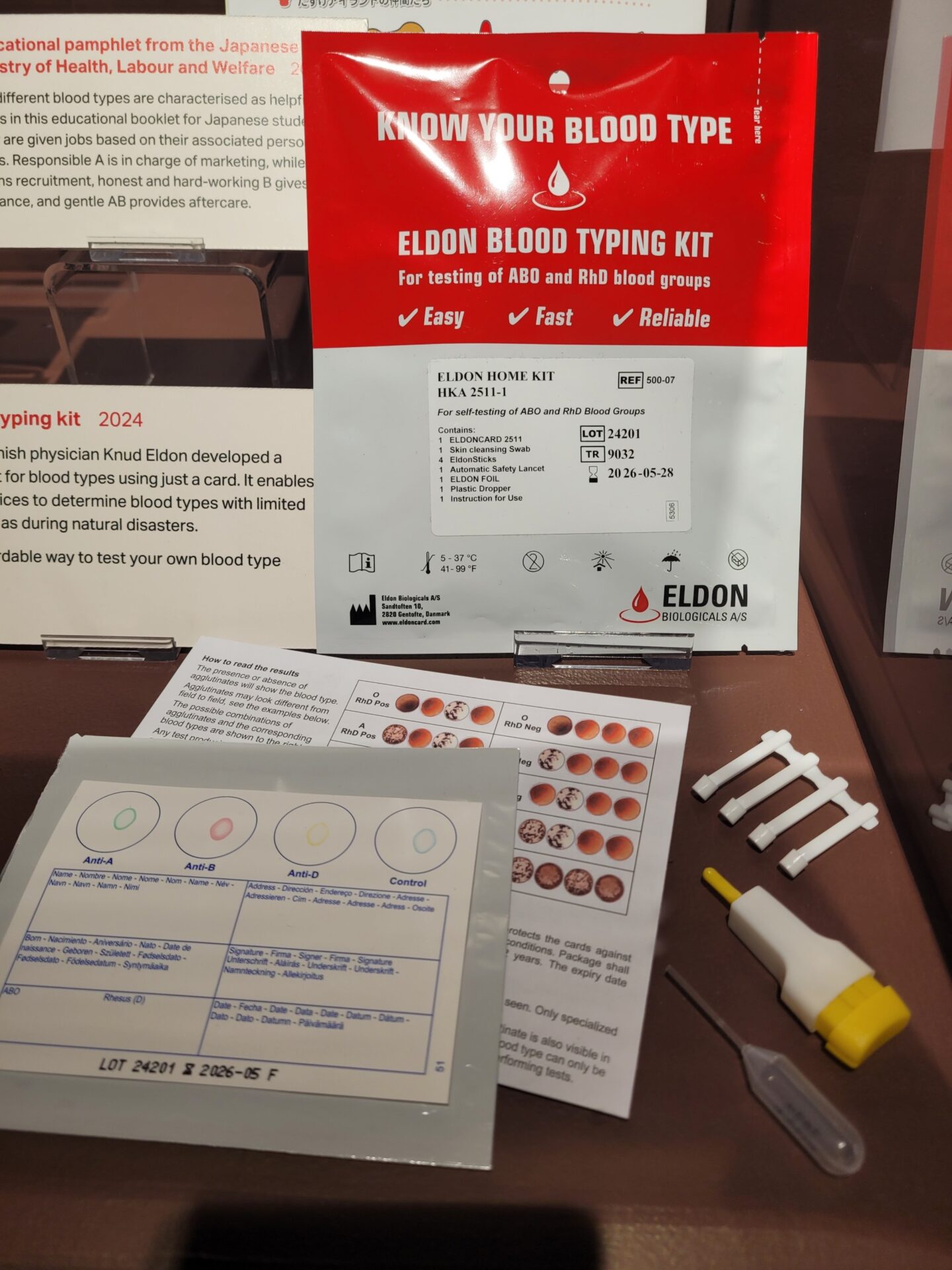
Did you know it is now possible to find out your blood type from the comfort of your own home? The Eldon Biologicals Blood Type Testing Kit allows you to test your own blood anywhere at any time. The toolkit is particularly useful for people living in countries prone to natural disasters, where emergency blood donations are required more often.
The Racialisation of Blood
During the mid-twentieth century, the American Red Cross was renowned for its continuous labelling of blood from Black donors. Despite protests from a variety of medical institutions and key political figures including First Lady Eleanor Roosevelt, the Red Cross appeared to value social typologies over scientific ones by continuing to racially segregate blood donations until 1948. For many medical institutions in this period, there remained a belief that race could be transmitted by blood. The American Red Cross’ response at the time was that this was more to do with concerns for soldiers receiving transfusions, rather than being based on scientific facts about blood.
Sickle Cell Disease (SCD) is an inherited health condition that affects the red blood cells. It is particularly common among people who originate from sub-Saharan Africa, the tropical region where malaria is endemic. Sickle Cell Trait evolved because it offered protection in this environment. Having the Trait does not mean you have the disease. If you do not inherit the trait from both parents, your health is generally not affected. It is only when you have two Traits that you develop the disease. In the US, SCD is the most commonly inherited blood disorder, impacting the lives of approximately 89,000 people. In the US census, people afflicted with SCD are primarily defined as being Black or African American. SCD is the forerunner of racialised ‘Black’ diseases. As such, it is often the case that SCD patients face unfounded prejudices when seeking treatment for their condition.
No One’s Listening: An Inquiry into the Avoidable Death and Failures of Car for Sickle Cell Patients in Secondary Care
Racist stereotypes associating Black people with drug abuse has plagued SCD services for many years. Patients with excruciating pain caused by the condition were often accused of being drug addicts when seeking treatment for an SCD crisis. SCD patients are still perceived as being opioid dependent at twice the rate of other patients with acute pain. Even the families and practitioners of SCD patients have observed that white SCD patients receive better treatment for their condition than Black patients do. Acute pain is a hallmark feature of SCD, any many patients report painful episodes starting in infancy.
‘Infected’ Blood
Different groups who have suffered due to associations with infected blood.
Haemophilia:
People with haemophilia have ‘different’ blood. Haemophilia is a condition where the blood does not clot properly. It is found almost exclusively in men. While some women do have the condition and can pass it onto their children, they rarely exhibit signs of illness.
‘My son, Jake was diagnosed with severe haemophilia A when he was eight months old. Shortly afterwards I found out that I was a carrier of the gene. I’ve come to realise that it doesn’t really matter how he got Haemophilia, it’s just something that’s happened that no one had any control over and what’s more important is how we manage it in our lives as a family. Our genes make up who we are and part of Jake’s genetic makeup is his Haemophilia and you know what, to me he is perfect!’
People with haemophilia were often the victims of stigma prior to the infected blood scandals of the 1980s. Physically, they suffered with chronic pain. Socially, they were often excluded from schools and jobs, and many struggled to participate in activities with their peers. The infected blood scandal only served to exacerbate these issues.
Due to their ‘unclottable’ blood, haemophilia patients require concentrates of plasma from blood products. Factor VIII blood products, obtained through paid donations in the US, were found to be infected with HIV and Hepatitis C.
The repercussions went far beyond the illness itself. Hospitals refused to treat the children of people with haemophilia despite them having proof that they did not have AIDS. Likewise, many children with haemophilia were required to prove that they were not infected to be able to attend school. The concerns of hospitals and schools were not unfounded: many men with haemophilia who were infected with HIV by these blood donations inadvertently transmitted the disease to their partners, who in turn infected their children.
Families of the victims were also often ostracised. Many partners of people who were infected were treated poorly in their workplaces. People with haemophilia were presumed to be gay because they had been infected with HIV, which was perceived of as a ‘gay disease’. In turn, many children who were infected were also labelled ‘gay’ rather than as victims of the disease, with one of the youngest victims dying of AIDS at 3 years old.
Some people who donated their blood were not aware that they were infected with Hepatitis C or HIV. Prisoners in the US and France were encouraged to donate their blood, despite many having been drug users. By donating their blood, they were seen to be moving towards social reintegration. Many donors were victims because they too were discovering their illness for the first time as a result of infected blood scandals. In addition to this, many people donated excessively due to their economic and other vulnerabilities that pressured them into selling blood. For example, in late-twentieth-century Japan, social outcasts and marginalised communities were often exploited into selling their blood. This procurement of blood reinforced social boundaries, and many blood banks became renowned for producing ‘bad blood’.
Many people who did not have HIV or had not donated blood were victimised simply because they were part of one of the communities associated with infection. This was particularly the case for homosexual and bisexual men. HIV and AIDS were portrayed to the public as a gay disease, rather than a medical epidemic. These men were subsequently banned from donating blood due to the association between AIDS and homosexuality. Many gay men saw this exclusion as a slur against homosexuality, which had only recently been declassified as a disease in 1979. They felt they were being stigmatised based on their identity, rather than their behaviour.
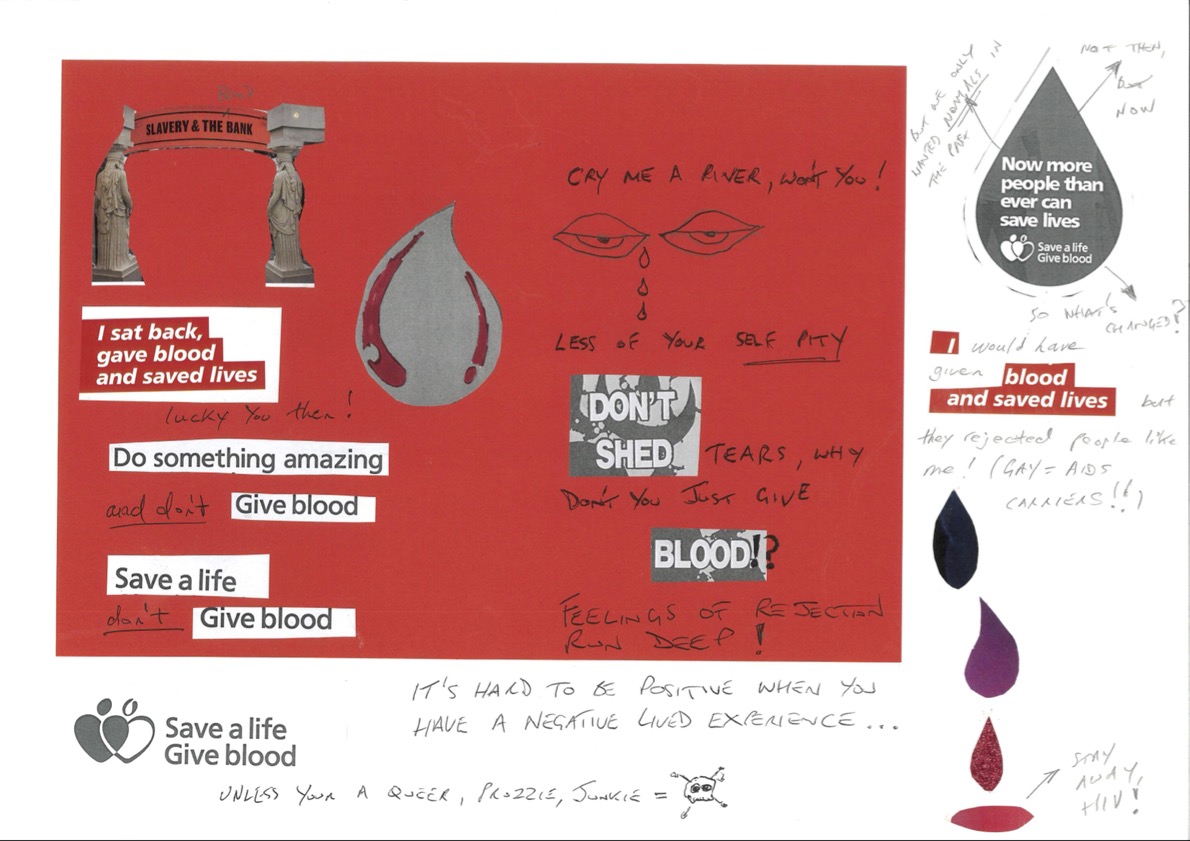
This poster, designed by a member of Thackray Museum of Medicine’s local community, represents the complex and emotional relationship between gay communities and blood donation. You can see more of our community-designed blood posters in Connections: Part 2.
Up until the infected blood scandals of the 1980s, homosexual and bisexual men had been some of the most active blood donors in a variety of communities. Another group excluded from donation as a result of the infected blood scandal were people from certain ethnic backgrounds, particularly African and Haitian communities. This association became a common theme in blood donation posters focused on AIDS. People from African communities or who had recently travelled to Africa were actively discouraged from donating blood in the UK via blood donation posters. In 1996, an Ethiopian Jewish community in Israel rioted after they discovered health authorities had secretly dumped their blood donations out of fear that their blood might be contaminated. This decision was made on the basis that the Ethiopian population had relatively high rates of AIDS.
Take a look at these Blood Sample Tubes.
These tubes contained CAT Serum Separator Clot Activator to catalyse the coagulation process, generally used for tests requiring a serum sample. One bears a yellow ‘Danger of Infection’ biohazard sticker of the type used by Leeds Teaching Hospitals until 2022 to label blood samples from HIV-positive patients.
How would you feel if your blood was labelled a ‘biohazard’?

Cancer
There are several types of cancer that affect the blood. These include leukaemia, lymphoma, and myeloma. Having ‘different’ blood due to cancer can affect people’s identity in various ways. Read about the experiences of blood cancer patients below.
Cell Division
I am the only person my blood can save.
All blood cells start out the same. Stem cells in your bone marrow are blank slates with the potential to become any part of your blood as they divide and grow. In just a few short weeks that baby stem cell can graduate into an infection-battling lymphocyte, a white blood cell with a vital role in a healthy immune system.
As I approached my own graduation, my white blood cells were not behaving in this normal way. While studying for my finals as a student, I was also undergoing a series of tests, scans and a biopsy that revealed my lymphocytes didn’t just divide into two neat new cells; they popped like a kernel of corn. That’s genuinely what it’s called – a popcorn cell – because under the microscope the cells look like misshapen bobbles of popcorn. Nobody really knows why your DNA can just decide to change like this. Sometimes it just does.
These inappropriately cheerily-named mutants are a sign of a rare blood cancer – nodular lymphocyte-predominant hodgkin’s lymphoma – which meant that the next few months were filled with a cycle of chemotherapy and recovery.
At the end of it, I gave blood the only way that I could: having my blood stem cells harvested for my future self. The probability that some of my cells remain cancerous means that I can never give blood for another person without risking infecting them. But I already have that cancer in me and, as nobody’s stem cells are a closer match with me than my own, it made sense for me to be the donor.
Taking stem cells is not as easy as regular, whole blood. A needle was driven right into the bone marrow in the back of my hip. And that is after I had been weakened by an extra-strength dose of chemo and spent the intervening days injecting myself with growth factor drugs.
The cells were frozen for a future transplant that never happened. I went into remission and recovered. But the whole process made me very aware of how the peculiarities of my blood had separated me from the normal chain of blood donors and recipients.
If donating and transfusing blood is all about sharing, connection and community, a precious gift to save the life of a stranger, then my bad blood means isolation from that imagined community. The value of blood to medicine and society is immeasurable, but the only person my blood has value for is me.
Different Bloods
In deciding which aspect of having a leukaemia I would offer for the museum records, its impact on my social life and very personal life appears to me to be the overriding impact of my blood cancer.
I have Chronic Lymphocytic leukaemia (CLL) and am fortunate to have the variety which though it has undesirable symptoms, means I am expected to die with it not of it.
For the first 10 years after diagnosis, I managed to live a fairly normal though curtailed life, avoiding things like plane journeys, and very crowded places which may have given me an infection. My leukaemia causes the immune system to become far less effective at fighting infections resulting in immune compromised status.
When Covid arrived on the scene 5 years ago its impact was immediate and heart breaking. My partner died and no one was able to be with me, so I dealt with his death and funeral alone when my family had expected and wanted to be with me.
I had planned how my days would get filled with activities to help me through the grief of losing one I loved so much. That was not to be, instead my days were spent alone, except for iphone contact with my lovely daughter and my dear sister in law, their caring gave me a reason to keep living.
Eventually the world seems to think covid has gone, for immune compromised people, especially elderly like me it can be a death sentence. For that reason family have to check they are well before they can visit, and days out, bus journeys, trips, concerts busy places, etc are not for me. I have become a hermit.
I buy FFP3 masks and now venture to shops, and other centres with them on, and spray anti-virus cold remedies up my nose hoping to defeat any viruses.
I am making some effort to live, as I have sold my home and moved to live near my daughter. Only people who live with this restrictive blood disease truly understand how dangerous the world is to us.
I am lucky, blood when it tries to destroy the body it inhabits causes pain to many, medicine has not beaten it yet, and what medicine there is comes with numerous debilitating side effects for many. This is what blood means to me.